
Trauma and Addiction: The Link We Can’t Ignore (Clinician Edition)

Every other day brings some news headline about a celebrity or politician struggling with substance use or an addiction disorder. Unfortunately, there are also countless news stories about dangerous drug trends or the lack of resources to deal with the ever-growing problem of addiction in the general population.
As a counsellor or professional working with clients facing addiction, you have witnessed the chaos, confusion, fear, and hopelessness that addiction causes.
Often, people view addiction as a "choice" – those addicted "choose" to use. Unfortunately, most counsellors have few clients living in the chaos of dependency who want to be there. They don't want to be dependent on substances – they likely do not know how not to use them. But what exactly creates the move into addictive patterns of substance use? What causes compulsive engagement in a particular unhealthy or life-threatening behaviour? The explosion of scientific discoveries based on neuroscience has made a profound contribution to our understanding of trauma and the impacts trauma has on the development of addiction and how people recover.
This article is for clinicians, counsellors, and mental health professionals. It helps make sense of the behaviours and consequences of addiction. But it is also about making sense of trauma - because trauma and addiction disorders connect in a way that needs to be understood. Research demonstrates that difficult life experiences often pave the way for a person to use substances or compulsive behaviours as a way to self-medicate. So a better understanding of why addiction happens and how trauma often contributes is a crucial place to start.
Research shows the importance of identifying and addressing trauma as part of the treatment plan for those experiencing addiction.
Understanding the vital connection between trauma and addiction helps provide our clients with a better foundation in their search for what helps them recover. So I hope you find something that allows you to offer trauma-informed tools to support those who are pursuing recovery from substance use and addiction disorders.
Here is what you will find in this article:
The Problem is the Problem
It shouldn't surprise us that substance use and addiction disorders have become one of the top health concerns in North America and around the world.
Substance use disorders (SUDs) are among the top public health concerns in North America and many other countries worldwide.
The economic cost of substance use disorders worldwide (including alcohol and other drugs) is staggering. In the US alone, the annual cost of substance use disorders is $442 billion. It includes costs associated with health care, social services, loss of productivity, and crime associated with substance addiction. (1)
About 1 in 10 North Americans over 15 report alcohol or drug dependence. These numbers are similar in many other countries. (2)
Besides substance use disorders, millions of people worldwide experience the painful consequences of behavioural addictions, including gambling, gaming, food, shopping, or pornography.
Most people who struggle with substance use or an addiction disorder never enter a treatment program.
Of those who seek some form of treatment, the vast majority will continue to struggle with the negative impacts of their disorder.
This information confirms what we already know: millions of North Americans live with the painful experience of addiction – and few get the help they need to recover.
Addiction Isn’t “The” Problem
Any effective treatment for a problem or issue begins with a clear understanding of the nature of the problem. Why do substance misuse and addiction problems develop in the first place? Why do attempts to stop often fail? What will ultimately help our clients recover?
One critical perspective that can get overlooked is that addiction is often a symptom of the problem rather than the problem itself. While addiction certainly creates additional "problems", we need to be curious about what drives the behaviours that lead to addiction in the first place. For many people who struggle with addiction, their excessive use of drugs, alcohol or other unhealthy coping behaviours likely started a way to "fix" some problem or pain.
What is the pain or the problem that substance use is trying to “fix”?
The answer to that question is a complex one. Gabor Maté, the author of "In the Realm of Hungry Ghosts" (3), encourages us to ask not about why addiction occurs but "why the pain?"
To understand what moves people in the direction of addiction, we need to explore the recent contributions of research across diverse topics, including neuroscience, genetics, addiction, and the impacts of trauma and chronic stress. Quite simply, we need to better understand the origins of addiction rather than just viewing it as "the problem".
If we keep seeing substance misuse and addiction as “the” problem that needs fixing, we are less effective in supporting people in their desire to move out of self-destructive patterns of addiction.
Addiction “Manages” the Problem: Trauma Symptoms
It's crucial to grasp two important things when trying to understand the seemingly baffling behaviours of substance use and addiction disorders.
Knowing how our nervous system is wired helps us better understand our thoughts, feelings, behaviours, body sensations, and automatic reactions. Understanding our nervous system helps us know what makes us human.
We need to recognize that difficult or traumatic experiences impact almost every aspect of someone.
Although not all addiction is caused by trauma or painful life experiences, we certainly have learned that trauma is a much more common experience, especially in the lives of those struggling with addiction. There is also a greater understanding of trauma's profound impacts on a person's physical, emotional, and mental well-being.
There has been a significant movement towards identifying and exploring the connection between trauma and addiction.
Many of our clients will assume (wrongly) that the term “trauma” does not fit their experience. They may see their painful life experiences as just a part of their life they wish to forget. For many, their challenging life experiences were just that – “life experiences”. Most people struggling with addiction seem quick to discount their experience – “that wasn’t trauma”, “that’s just the way it was”, or “other people have had it far worse”.
Research into the origins of addiction points us towards the impacts of adverse childhood experiences and the effects of chronic stress and other sources of trauma. Peter Levine, a renowned psychologist in treating trauma, argues that it is detrimental for someone to be unaware of trauma's negative impact on their lives. (4)
Not knowing they were traumatized doesn’t prevent someone from being negatively affected by their experiences.
Trauma and Its Connection to Addiction
Addiction research identifies trauma as a significant contributing factor to substance use and addiction patterns. Current research shows us that traumatic experiences, especially in early life, create a greater vulnerability to developing substance abuse problems.
Here are some statistics from a variety of sources that show just how significant this connection is:
In North America, the percentage of people diagnosed with Post-Traumatic Stress Disorder (PTSD) throughout their lifetime is close to 7%. (5) In the substance-dependent population, this percentage increases dramatically – various studies show that 25-42% of people receiving treatment for substance use disorder also have PTSD. (6)
Dr. Edward Khantzian, a Harvard Medical School researcher, developed the self-medication hypothesis of substance abuse. (7) His research demonstrates that people with PTSD are four times more likely to develop problems with substance use than those without a PTSD diagnosis. A history of childhood trauma also leads to using substances earlier and more problematic substance use overall.
The National Comorbidity Study shows that individuals with PTSD are 2 to 4 times more likely to have a substance use disorder than those without PTSD. The research from this same study also suggests that trauma is more likely to occur before drug or alcohol misuse than after it happens. (8)
This research encourages us to consider that traumatic events often contribute to the development of substance use and addiction disorders. Even if someone doesn't meet the criteria for an official diagnosis of PTSD, it is still essential to recognize that trauma may still affect their lives and substance use patterns in significant ways. In fact, early childhood trauma symptoms rarely fit the diagnostic criteria of PTSD even though the traumatic experiences may have been extensive.
We need to be open to considering that addiction is often just one of the symptoms of “the problem”: unidentified or unresolved trauma.
Shifting our perspective allows for more compassion and support for those who want to make lasting and positive changes in unhealthy substance use and addiction patterns.
Why People Mood Alter with Substances or Behaviours
If we want to help people with addiction pursue recovery, we need to pay attention to how often trauma is both an unspoken and unacknowledged experience for many of them. The consequence of missing this critical connection adds to the struggle for those stuck in addictive patterns.
Researchers have developed many different theories about why some people become addicted to their substances. For example, genetics, brain chemistry, social norms, and personality traits contribute to addiction patterns. But the life stories of those in addiction reveal an obvious pattern – most have had painful and overwhelming life experiences.
While not everyone who has experienced trauma moves into addiction, most people who struggle with addiction have been through challenging or traumatic life experiences. As therapists and mental health workers, we have heard the stories. Current trauma-informed research has led to a much greater understanding of trauma's impact on the development of addiction issues.
Most would agree there is an increased risk of trauma for heavy substance users, including accidents and injuries, exposure to violence and sexual trauma, and substance-related illnesses. People struggling with addiction also experience more traumatic losses.
While the high risks associated with substance use can be a source of trauma, most people who experience both trauma symptoms and substance dependence were exposed to significant adverse experiences long before their misuse of substances began.
Trauma symptoms differ significantly from person to person, but common trauma symptoms include increased anxiety, fear, anger, and shame. Some people experience insomnia, nightmares, mood swings, agitation, or difficulty concentrating following a traumatic experience. Sometimes a person remains on "high alert" following traumatic experiences, or they may be jumpy and easily startled. A person might feel more disconnected from themselves or others. There may also be particular situations or places that trigger extreme emotional reactions.
Those experiencing addiction are often anxious, have difficulty managing their emotions, or tend to be impulsive. In addition, complaints such as insomnia are frequent. But it is not helpful if we only attribute these experiences to a person's use of substances or the chaos of life in addiction.
It is far too easy to mistake some of the common symptoms of unresolved trauma for the negative consequences of substance use.
When we miss the connection between trauma and substance use, we risk seeing their struggles as resulting from their own choices and behaviours. When that happens, we will fail to provide the resources they need to deal with the underlying impacts of trauma. The process of recovery is already fraught with enough challenges.
Adverse life experiences leave a legacy of unmanageable trauma symptoms. The more someone experiences the ongoing disruptions of trauma symptoms, the more likely they will gravitate to substances and behaviours that help them mood-alter and self-medicate.
Although it is essential to acknowledge the strong correlation between trauma and substance use, it is also necessary to understand why this link is so pervasive. There is a simple explanation for this high rate of connection between trauma symptoms and SUDs that requires a closer look:
People are self-medicating their dysregulation and trauma symptoms by using substances or behaviours.
Many clinicians recognize that the use of potentially addictive substances and behaviours often began as a coping mechanism for mental health and trauma symptoms. For example, the US Substance Abuse and Mental Health Services Administration recognizes the impact of trauma and how it increases the risk of substance misuse.
“A trauma-informed perspective views trauma-related symptoms and behaviors as an individual’s best and most resilient attempt to manage, cope with, and rise above his or her experience of trauma.” (SAMHSA) (9)
Here is some research that helps us understand the connection between challenging life experiences and addiction disorders:
The Self-Medication Hypothesis
The Self-Medication Hypothesis was developed over 30 years ago by Dr. Edward Khantzian and his colleagues at the Harvard Medical School. (10) Over the years, this research has contributed to our understanding of substance use and addiction disorders, especially in medicating overwhelming emotions and experiences. His goal was to understand what drives behaviours that seem so self-destructive.
Dr. Khantzian concluded that the heart of addictive disorders is suffering, not a "reward" or seeking pleasure – addiction is about self-medicating distress and painful feelings.
He believed that addiction problems are less about pleasure-seeking, reward, or self-destructiveness than human psychological vulnerabilities. Addictive substances may help relieve emotional pain, but these attempts to self-medicate are short-lived.
Dr. Khantzian proposed that addiction is a combination of poor emotional regulation skills, genetic vulnerability, and environmental influences. In developing the Self-Medication Hypothesis, he also observed that those with addiction have difficulty regulating emotions, including the overwhelming and intolerable feelings that trauma produces.
Those in addiction also experience challenges with their sense of self-worth, their relationships, their behaviours, and how they practice self-care. Khantzian notes that the widespread availability of addictive substances to relieve distress only re-enforces the use of drugs or alcohol. He sees addiction as a "self-regulation disorder" – substance users perpetuate their suffering in an attempt to control it. But continued substance misuse only makes the challenges with self-regulation worse.
Addictive drugs and behaviours help relieve overwhelming distress, but attempts at self-medication are short-lived and often replaced by suffering associated with addiction.
Adverse Childhood Experiences (ACE) Study
The Adverse Childhood Experience Study (ACE Study) (10) is vital research that also supports the concept of substance misuse and other behaviours like smoking or disordered eating to manage the overwhelming experiences of childhood trauma. In the 1990s, Vincent Felitti and Robert Anda spearheaded a ground-breaking study of over 17000 participants that looked at the association between adverse childhood experiences and the health or social problems experienced as an adult.
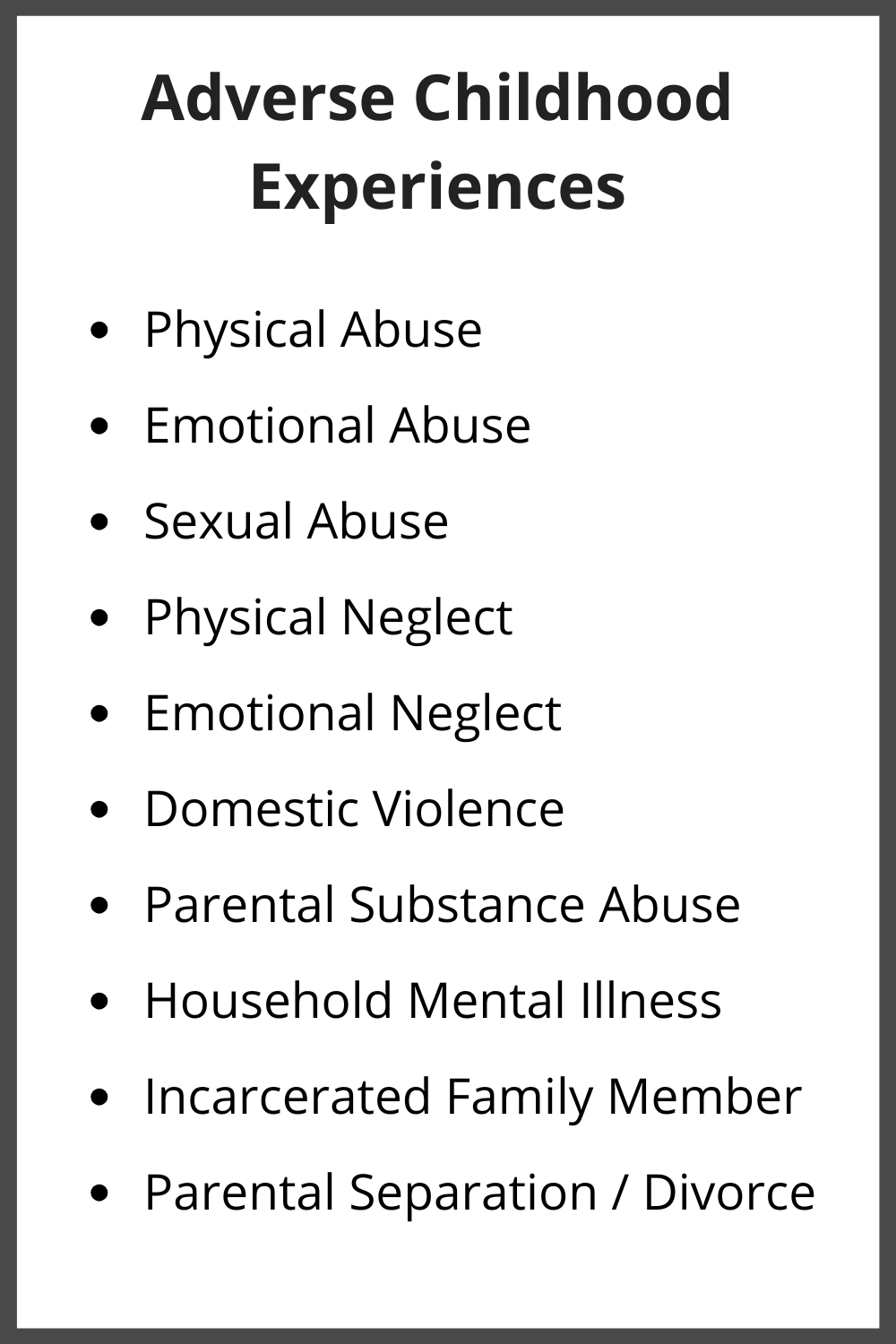
The researchers began by identifying ten specific categories of common childhood trauma that included physical, emotional, and sexual abuse, physical and emotional neglect, and family challenges, including parental separation, addiction, mental illness, violence, or incarceration. Next, adult participants were asked how often they experienced these types of trauma in their childhood. Then, they were asked to identify the physical and mental health concerns they had as adults.
The information they gathered from this extensive survey provides us with a clear picture of the negative impacts of painful life events in the lives of children. Moreover, this study shows that adverse childhood experiences are vastly more common than previously thought.
The ACE Study identifies the progression that leads to the health concerns and social problems seen in adults who have experienced childhood trauma. It demonstrates that children who experience adverse childhood experiences (ACEs) experience emotional, social, or learning challenges. As a result, they adopt unhealthy and high-risk behaviours (including heavy substance use) to cope, which leads to increased social problems, health issues, disabilities, and early death.
We need to understand what often happens to children who grow up in traumatizing family situations. Adverse childhood experiences create more difficulties in managing anger or anxiety. Kids who grow up experiencing trauma tend to act out more. As a result, they have more trouble relating to their peers – they often get bullied or act aggressively towards their peers.
And, because their brains are more focused on surviving difficult situations, they often struggle in school. As a result, these kids start engaging in unhealthy and high-risk behaviours (including substance use) to connect with others or cope with the stressors they are experiencing. These unhealthy behaviours then lead to more social problems, more challenges with learning, health issues, and disabilities. As clinicians, we often see this cycle demonstrated in the lives of those who have substance use or addiction disorders.
Although the statistics from the ACE Study indicate that 33% of all participants reported no significant adverse childhood experiences, at least 17% reported experiencing three or more categories of ACEs. The statistics regarding the association between the number of ACEs and the challenges encountered in adulthood are staggering.
Those who have experienced four or more ACEs are between 4 and 12 times more likely to have an alcohol or drug use disorder than someone with an ACE score of zero. (11)
In fact, the highest risk of self-reported alcohol problems (30.7%) was reported by those who experienced four or more ACEs and a history of parental alcoholism. (12) Let this statistic sink in because it has significant implications for understanding the development of an alcohol use disorder. There is a common belief that alcohol addiction has a substantial genetic contribution. While there may be a genetic component, let's not underestimate the profoundly negative impact growing up with a parent with alcohol addiction has on a child. Being parented by someone with an addiction is a traumatic experience for children.
To believe that addiction is mainly genetic minimizes the harmful impacts of growing up in a home where addiction is present.
As clinicians, we must help our clients identify how many of these categories of ACEs they experienced in their childhood. Their “ACE Score” is how many of these 10 types of adverse childhood experiences they faced in their childhood.
Suppose a client has been through one or more of these adverse childhood experiences and has substance use issues or addiction challenges. In that case, they might be using substances or behaviours to help them cope with the negative impacts of those experiences.
They might use their drug or behaviour of choice to help them feel less anxious, less irritable, or less angry. Drugs or alcohol might help them fall asleep or dampen an excessive startle response. They may also use them to stop intrusive trauma-based thoughts or memories.
Substances might help them disengage from the parts of life that are overwhelming. For example, those with trauma histories are far more likely to use substances or addictive behaviours as a form of emotional avoidance – to numb painful feelings associated with traumatic experiences or traumatic memories. These are just some ways that addictive substances and behaviours may help “manage” the pain associated with a past trauma history.
In summary, for many people, addictive patterns are often a way of dealing with distress – it is a behaviour that begins out of pain. Essentially, they are medicating common trauma symptoms.
Self-Medicating Trauma Symptoms
Gabor Maté, the author of "In the Realm of Hungry Ghosts", calls addiction a "flight from distress". He believes this:
Addiction originates with pain, especially the pain of early trauma and abuse – addiction is the emotional anaesthetic. (13)
Many clinicians agree that traumatic experiences and the painful imprint on emotions, memories, relationships, and the nervous system motivate people to use substances or behaviours to self-medicate. For example, John Briere states that individuals with complex and chronic trauma histories are more likely to use drugs and alcohol as an emotional avoidance – substances numb painful feelings associated with traumatic experiences or traumatic memories. (14)
But there are many complex reasons people self-medicate that are not simply about numbing emotions or memories. Trauma symptoms can be quite diverse in their presentation - people are impacted in different ways depending on the nature of the trauma, their age, the resources available to help them cope, or the sheer number of adverse experiences some have faced.
Recent advances in addiction treatment have come from increased awareness and understanding of trauma, trauma-related symptoms and how they impact the move into substance use and addiction. Research including the ACE Study (10) has made this link undeniable.
Trauma has made a profound contribution to the development of substance use and addiction disorders for the vast majority of those who experience addiction. But unresolved trauma also contributes to patterns of relapse, especially when trauma-related symptoms have not been adequately identified or addressed in treating addiction.
It is crucial that clinicians identify and assess trauma symptoms that often contribute to someone’s patterns of addiction.
Two Categories of Trauma Symptoms that Addiction “Solves”
There are many different ways trauma leaves its "fingerprints" on who someone is and how they function. These impacts are easier to identify if we view trauma as being more about how a traumatic experience continues to impact someone after the event has passed rather than just thinking about trauma as an event that occurred. And these symptoms are also easier to understand if we think about them in terms of how trauma impacts our nervous system.
It is helpful to define the "nervous system" if we want to make sense of trauma's impacts on it. This system includes the brain, spinal cord, and nerve systems throughout the human body. Essentially, it controls everything a person does. This basic operating system controls thoughts, feelings, instincts, bodily functions, and bodily sensations.
Trauma symptoms generally fall into two basic types. Trauma researchers often classify symptoms as being "bimodal" – having two distinct ways these symptoms are experienced. One category is "hyper-arousal" symptoms related to the increased activation of the fight or flight response following trauma or stress. There is often too much activation or energy in the nervous system. The other category is "hypo-arousal" symptoms – it is more related to the freeze response of trauma and includes such experiences as numbing, shutting down, and dissociation. (15)
1. Hyper-arousal: High Activation, Intrusive Experiences, and Fear
The term "hyper-arousal" describes the high level of activation that remains in the nervous system and the physical body following a traumatic experience. It is an ongoing activation of the fight or flight response even after the threat or the trauma has ended. Some people continue to live in this state of high trauma activation long after the trauma has passed. This highly activated state profoundly impacts their experience of themselves and their world.
When high activation in the nervous system remains following a trauma, it contributes to the development of trauma symptoms that fall into the hyper-arousal category.
Another way to describe hyper-arousal is that there is too much of a vast number of uncomfortable symptoms, including:
The Nervous System is on High Alert: A person may be jittery or startle easily, more reactive, more impulsive, and experience more significant irritability or even aggressiveness. Hyper-vigilance becomes a way of being in the world – they are always watchful for any sign of potential threat. Sleep becomes difficult. (16) When nervous system activation is high, it also makes learning difficult.
Physical Symptoms: When the nervous system remains on “high alert”, the body also remains on high alert. A person can experience overwhelming bodily sensations following trauma if the physical manifestations of the fight or flight response continue after the danger has passed. (15) Some of the physical symptoms include tension and stomach upset and all the physical manifestations of a fear response.
Re-experiencing Symptoms: These profoundly disturbing experiences include trauma-based flashbacks, nightmares, and intrusive images. Intrusive experiences are ways that a person continues to relive their original trauma.
Emotional Reactivity: The ongoing emotional experience following trauma can be one of reliving the primary emotions of trauma, including heightened anxiety, fear, horror, shame, and anger. There can also be a greater struggle with expressing anger in appropriate ways.
Self-Destructive Behaviours: Trauma also leads to self-destructive behaviours that can be an attempt to manage the overwhelming experience of high activation – self-harm, disordered eating, compulsive sexual activity, and substance misuse become common experiences. (15)
Impacts on Physical Health and Mental Health: The ACE Study demonstrates a clear connection between a history of childhood trauma and chronic health or mental issues in adulthood. (10) Trauma researchers have demonstrated a link to specific disorders that stem from the nervous system's hyper-arousal state, including anxiety, cardiovascular issues, and digestive disorders. (15)
2. Hypo-arousal: Avoidance, Numbing, Disconnection and Dissociation
"Hypo-arousal" is used to describe different post-trauma experiences. Rather than a state of high activation experienced through the "too much" symptoms of hyper-arousal as listed above, hypo-arousal symptoms show up as a state of disconnection, numbing, and avoidance. It is the "too little" category of symptoms. "Dissociation” or “immobilization” are clinical words often used to describe this state of shutdown. If the hyper-arousal state is the "fight or flight" response, the hypo-arousal state is the "freeze" response.
Hypo-arousal symptoms show up as a state of dissociation or disconnection that results when trauma and traumatic stress become too overwhelming, and the nervous system moves into an immobilized or “freeze” response.
Peter Levine acknowledges dissociation in traumatic experiences helps make the unbearable bearable. He describes this freeze response as similar to the accelerator and the brake applied simultaneously, creating forceful turbulence inside the body that produces the "hypo-arousal" symptoms of traumatic stress. (4) This type of response occurs without conscious thought – it is an instinctive response to an overwhelming experience. And it occurs, in part, as a way of buffering against the painful experiences of trauma symptoms.
When this high level of trauma activation in the nervous system results in a “freeze” response, it contributes to the development of trauma symptoms that fall into the hypo-arousal category. This “too little” category of symptoms includes:
Emotional Numbness: There is a sense of being emotionally numb, detached, or empty. A person might feel out of touch with their emotions. It is a way of protecting against painful or overwhelming feelings. For some, this numbness happens automatically. For others, substances or behaviours help create emotional numbness. The downside of numbing painful emotions is that it blunts the positive or enjoyable ones, which also adds to why people mood alter.
Relational Avoidance and Isolation: Traumatic experiences can create a tendency for someone to withdraw and isolate. Unresolved trauma, primarily relational trauma, can create more discomfort with connection. Instead, a person can develop patterns of avoiding intimacy, vulnerability, or contact with other people.
Physical Symptoms: The "too little" symptoms that impact the body include having little or no energy to complete daily tasks. The experience of fatigue or exhaustion is common. In addition, trauma can affect the ability to feel sensations in the body.
Behavioural Symptoms: Those who learned to cope with trauma by dissociating or shutting down often continue to respond in similar ways when they face stress. (15) They are more likely to freeze in challenging interactions or withdraw from social interactions that feel overwhelming. Hypo-arousal and dissociation are also significant contributors to mood-altering and addiction. Some people counter the pervasive experience of numbness and detachment by engaging in sensation-seeking in dramatic ways, including high-risk substance use and behavioural addictions such as sexual acting out and excessive gambling.
Impacts on Physical Health and Mental Health: Just as there are physical and mental impacts of living with a chronically hyper-aroused state in the nervous system, there are health and mental health issues that come from living in a state of hypo-arousal. Some of these challenges include depression, alexithymia, and chronic fatigue. (17)
Substance Use and the Symptoms of Trauma
The use of mood-altering substances and compulsive behaviours is common among those who have been through traumatic experiences and continue to suffer from ongoing trauma symptoms. For those who experience a constant sense of reliving their trauma and living in a state of hyper-arousal and the high activation of a chronic fight or flight response, it is no wonder they might seek out options to help them shut down or numb out. (5) Others use substances to counter the numbness and detachment they experience in the hypo-arousal state. Research also defines substance abuse as an attempt to bring a sort of "chemical dissociation".
Willie Langeland and his colleagues were some of the first researchers to study the concept of chemical dissociation. Their research points out that some substance users may have a more limited ability to dissociate in the truest clinical sense. So they likely rely on mood-altering substances to produce a dissociative state.
“Traumatized individuals with limited capacities to psychologically dissociate may attempt to produce similar soothing or numbing effects by using psychoactive substances. These substances are used to enter and maintain dissociative-like states.” (18)
Although dissociative states tend to "feel better" than the state of high activation and hyper-arousal, they are certainly not healthier. Instead, they only bring further damage and numbing resulting from an ongoing disconnection from more beneficial resources, coping tools, and relationships. For many people who struggle with addiction, substance misuse began as an attempt to fix a problem that was created through trauma.
Clinicians must understand addiction is often a symptom of the problem rather than the only problem that needs addressing.
Some Final Thoughts
Substance use and addiction disorders are common among those who have been through traumatic experiences, especially when they continue to suffer from ongoing trauma symptoms. So it is no wonder they might seek out options to help them shut down or numb out. Others use substances to counter the numbness and detachment they experience.
For those who've had trauma, addiction is a way to dampen the pain. Let's remember that substance use and other addiction disorders began as an attempt to fix a problem that trauma created.
Trauma-informed care recognizes the principles of safety and compassion are foundational to the process of healing and recovery for anyone experiencing a substance use disorder, especially when trauma has been a contributing factor.
I appreciate your interest in "Trauma and Addiction: The Link We Can't Ignore", written specifically for mental health and addiction professionals. I am grateful to have an opportunity to do my part in bringing more compassion and more science to the field of addiction recovery. I hope this article has encouraged you to explore further ways to support clients in addressing their addiction disorder and any traumatic experiences that may have contributed.

If you found this article helpful, here’s another resource for you.
Take a look at the free e-Book written for general audiences. It’s a great resource for anyone.
References
(1) Office of the Surgeon General: Addiction and Substance Misuse Reports and Publications https://www.hhs.gov/surgeongeneral/reports-and-publications/addiction-and-substance-misuse/index.html
(2) Recovery Research Institute https://www.recoveryanswers.org/research-post/1-in-10-americans-report-having-resolved-a-significant-substance-use-problem/
(3) Maté, Gabor. In the Realm of Hungry Ghosts: Close Encounters with Addiction. 2008.
(4) Levine, Peter A. Waking the Tiger: Healing Trauma: The Innate Capacity to Transform Overwhelming Experiences. 1997.
(5) National Institute of Mental Health. https://www.nimh.nih.gov/health/statistics/post-traumatic-stress-disorder-ptsd
(6) Weiss, N., M. Tull, M. Anestis, and K. Gratz. "The Relative and Unique Contributions of Emotion Dysregulation and Impulsivity to Posttraumatic Stress Disorder among Substance Dependent Inpatients." Drug and Alcohol Dependence 128.1-2 (2013): 45-51
(7) Khantzian, Edward J. "The Self-Medication Hypothesis Revisited: The Dually Diagnosed Patient." Primary Psychiatry Archive (2003). Primary Psychiatry. 2003.
(8) Coffey, S. F., J. P. Read, M. M. Norberg, S. H. Stewart, and P. Conrod. "Posttraumatic Stress Disorder and Substance Use Disorder: Neuroimaging, Neuroendocrine, and Psychophysiological Findings." Anxiety and Substance Use Disorders the Vicious Cycle of Comorbidity. 2008.
(9) Substance Abuse and Mental Health Services Administration (US); 2014. (Treatment Improvement Protocol (TIP) Series, No. 57.) Chapter 1, Trauma-Informed Care: A Sociocultural Perspective. Available from: https://www.ncbi.nlm.nih.gov/books/NBK207195/
(10) Felitti, Vincent J.; Anda, Robert F.; Nordenberg, Dale; Williamson, David F.; Spitz, Alison M.; Edwards, Valerie; Koss, Mary P.; Marks, James S. "Adverse Childhood Experiences". American Journal of Preventive Medicine. 14 (4): 245–258. (1998)
(11) McKenzie, Lynn LeTendre & Mark B. Reed. The Effect of Adverse Childhood Experience on Clinical Diagnosis of a Substance Use Disorder: Results of a Nationally Representative Study, Substance Use & Misuse, 52:6,689-697. (2017)
(12) Dube, Shanta & Anda, Robert & Felitti, Vincent & Edwards, Valerie & Croft, Janet. Adverse childhood experiences and personal alcohol abuse as an adult. Addictive behaviors. 27. 713-25. (2002)
(13) Maté, Gabor. In the Realm of Hungry Ghosts: Close Encounters with Addiction. 2008.
(14) Briere, J., and J. Spinazzola. "Phenomenology And Psychological Assessment Of Complex Posttraumatic States." Journal of Traumatic Stress. 2005: 401-12.
(15) Van Der Kolk, B. The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. 2014.
(16) Luxenburg, T., J. Spinazolla, and B. A. Van Der Kolk. "Complex Trauma and Disorders of Extreme Stress (DESNOS) Diagnosis, Assessment: Part One." Directions in Psychiatry 21 (2001): 373-92. Trauma Center at JRI. 2001.
(17) Scaer, Robert. The Trauma Spectrum: Hidden Wounds and Human Resiliency. 2005.
(18) Langeland, W., N. Draijer, and W. Van Den Brink. "Trauma and Dissociation in Treatment-seeking Alcoholics: Towards a Resolution of Inconsistent Findings." Comprehensive Psychiatry 43.3. 2002.