
The Vortex of Addiction: A Summary About How People Get Stuck (and How They Heal)
Addiction often feels like being pulled into a vortex—patterns that start as coping can become harder and harder to escape. This short overview explains the Vortex Model of Addiction through a trauma-informed, nervous-system lens, and offers a hopeful map for recovery.
Addiction involves being drawn into patterns that become harder and harder to escape. Over time, substance use and compulsive behaviors can cause serious damage to health, relationships, finances, and a person’s sense of self.
One of the most painful realities of addiction is that wanting to stop isn’t always enough. Many people feel confused by their own actions, genuinely desire change, but keep repeating the same behaviors.
The Vortex Model of Addiction provides a compassionate understanding of why this occurs. Instead of seeing addiction as a moral failure, it explains it as a coping mechanism driven by the nervous system—especially when trauma, chronic stress, or emotional overwhelm have shaped someone’s life.
The Core Idea
When life becomes too overwhelming—emotionally, physically, or relationally—people naturally seek relief. Substances and mood-altering behaviors often start as attempts to:
calm anxiety
shut down emotional pain
escape shame
reduce distressing thoughts
manage uncomfortable internal states
At first, these strategies may seem to “work.” However, over time, they often intensify dysregulation and disconnection—pulling a person further into the vortex.
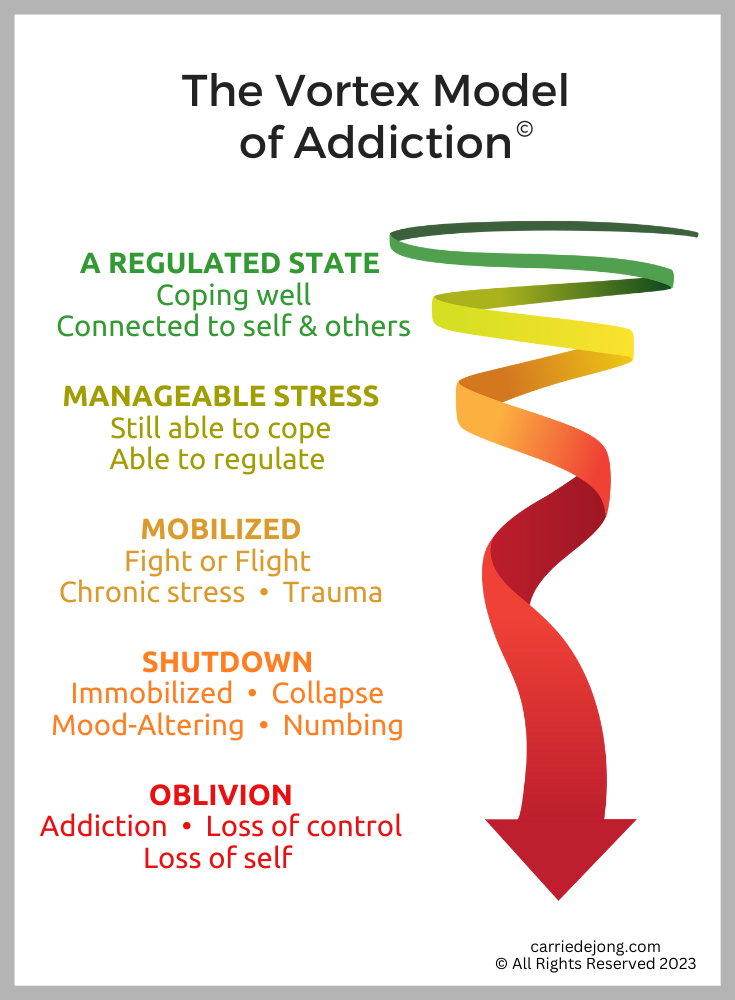
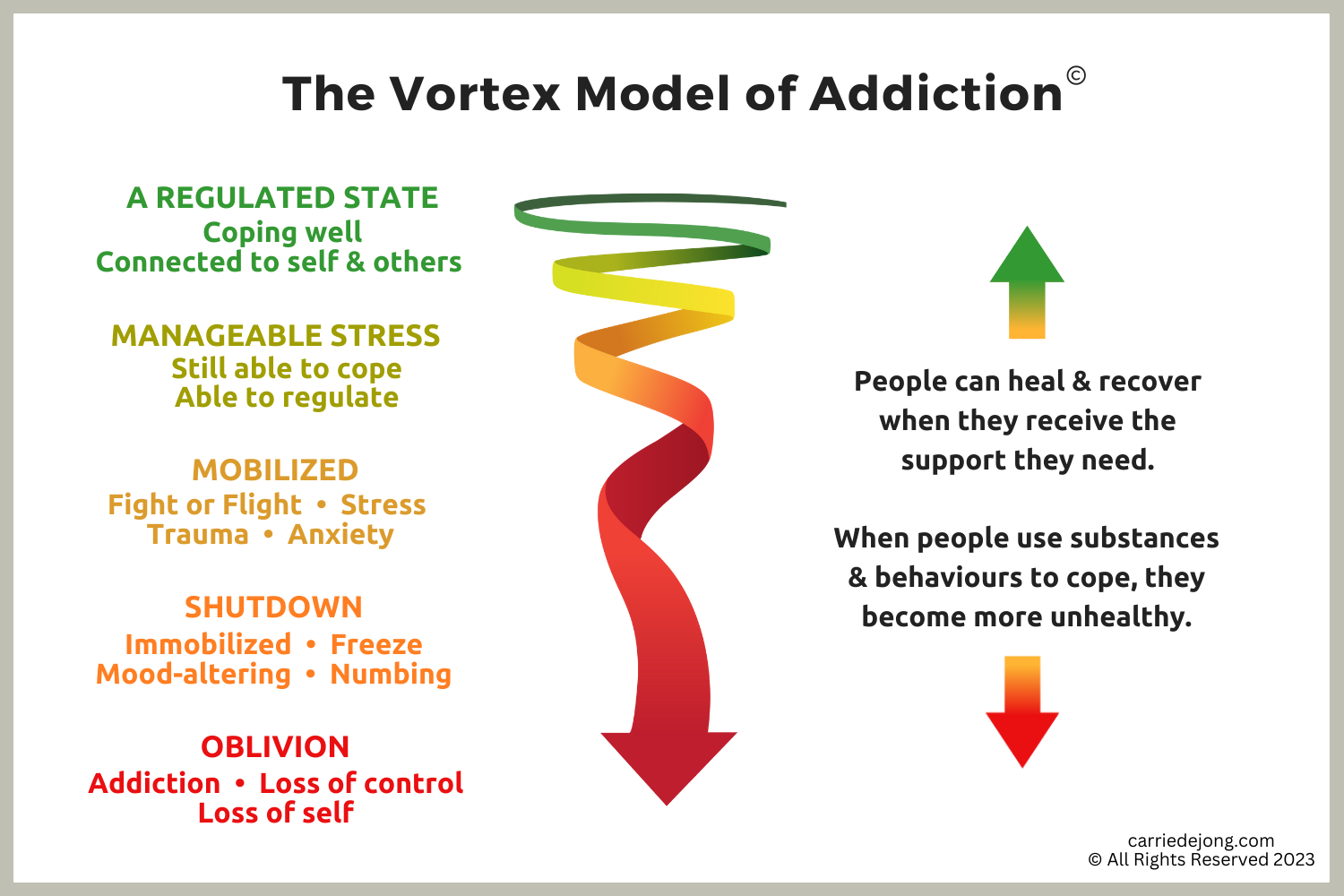
The Three States of the Vortex
1) Mobilized (Fight / Flight)
In this state, the nervous system is activated. People often feel:
anxious, keyed up, or on edge
restless, wired, or irritable
overwhelmed by stress
unable to sleep or settle
stuck in overthinking
In mobilization, substances and behaviors are often used to “take the edge off” or distract from distress. Common examples include:
alcohol
stimulants
excessive caffeine
compulsive exercise
gambling, shopping, gaming, or other high-intensity behaviors
2) Shutdown (Freeze / Numb)
When mobilization becomes too exhausting, the nervous system may shift into shutdown. People often feel:
numb or disconnected
emotionally flat
depressed or withdrawn
detached from their body
isolated from others
In shutdown, substances and behaviors are often used to:
stay numb
avoid pain
deepen disconnection
or temporarily feel something when life feels empty
3) Oblivion (End-Stage Addiction)
Oblivion is the stage where addiction becomes profoundly destructive. It may involve:
severe health decline
homelessness
overdose risk
substance-induced psychosis
suicidal thinking
major losses
a deep loss of identity and self
At this stage, people often cannot recover without significant intervention and support.
Why the Vortex Matters
The Vortex Model helps explain something essential:
Addiction is rarely about pleasure for long.
More often, it becomes about relief—relief from anxiety, pain, shame, trauma symptoms, or unbearable internal distress.
This model also shows why trauma and addiction need to be treated together. When trauma stays unresolved, recovery is more difficult. And when addiction persists, trauma symptoms often get worse.
The Way Back
Recovery is possible—and it often begins with support.
The path out of the vortex usually involves:
medical care when needed
addiction treatment and recovery supports
trauma-informed therapy
nervous-system regulation tools
safe relationships and community
rebuilding meaning, identity, and hope
Addiction may feel like a vortex, but healing is not only possible—it happens every day. With the right support, people can move back toward balance, connection, and a fuller sense of self.
Continue Exploring
A deeper look at the reinforcing cycles of addiction.
The biological processes that strengthen addictive behavior.
How a disconnection from self and others contributes to addiction.