
The Vortex of Addiction: Why Substance Use Becomes So Hard to Escape
This article presents a trauma-informed model of addiction that explains why substances become coping tools—and how recovery becomes possible.

Anyone caught in the vicious cycle of addiction can appreciate the term “vortex” as a way to describe their experience. Addiction is chaotic and painful. It involves the destructive use of substances or behaviors—and leaves significant harm behind.
Over time, addiction can damage physical and mental health, relationships, finances, career prospects, and even one’s sense of self. People who have experienced the grip of addiction often describe feeling pulled deeper into something they cannot escape. And one of the most heartbreaking realities is this: an honest desire to stop doesn’t always lead to lasting change—no matter how strong the wish for recovery might be.
There are many theories about what contributes to substance use and addiction disorders. Genetics, family history, social influences, and mental health all can play a part. Sadly, addiction is also often judged morally: that people are lazy, selfish, irresponsible, or simply seeking pleasure.
But what if there is a better way to understand addiction—one based on compassion and science? What if addiction makes sense when we understand what happens in the brain and nervous system under stress? That is what the Vortex Model of Addiction aims to do.
This model shows how circumstances, life events, and nervous system responses to overwhelming experiences help explain the transition into addiction. It also offers a framework for understanding how people become trapped—and what can support their return to recovery.
A note before we start: This is a longer, detailed article. If you’re currently struggling, please take your time with it. Some sections might feel intense. Make sure you take care of yourself and reach out for support if needed.
A Quick Map of Where We’re Going
In this article, you’ll learn:
how trauma, stress, and dysregulation contribute to addiction
why substances and compulsive behaviors often begin as coping tools
the three primary states of the Vortex Model: Mobilized, Shutdown, and Oblivion
how addiction develops over time
why recovery often needs support, not just willpower
Laying the Groundwork
I’m grateful to share this model of addiction, developed over nearly 30 years of clinical work as a counsellor in this field. Before I explain the model itself, it’s important to lay the groundwork.
My understanding of addiction has been shaped by:
the research of clinicians and scientists
the growing knowledge of the human brain and nervous system
an expanding field of trauma-informed care
newer approaches to healing trauma, including body-based therapies.
The Link Between Trauma and Addiction
Many of the articles I’ve written focus on the connection between trauma and addiction. My eBook, Trauma and Addiction: The Link We Can’t Ignore, explores this topic in depth. It explains how painful life experiences can pave the way for using substances and behaviors to self-medicate the common impacts of trauma.
Research shows that someone with PTSD is four times more likely to struggle with substance misuse than someone without PTSD.¹ Trauma isn’t always a contributing factor, but we know that adverse life experiences significantly increase the risk. The Adverse Childhood Experiences (ACE) Study reveals a strong link between traumatic childhood experiences and addiction.²
For anyone with a history of trauma and addiction, these two issues must be addressed together. When trauma remains unaddressed, recovery from addiction becomes harder. And when addiction persists, trauma symptoms often worsen.
Substance use often begins as a way to manage the overwhelming impacts of trauma, including anxiety, shame, intrusive thoughts, and uncomfortable physical sensations.
Ongoing Neuroscience and Trauma Research
The Vortex Model of Addiction draws from the work of many well-known researchers in trauma and neuroscience. Over the past two decades, researchers have offered profound insight into how the brain and nervous system are wired—and how they are affected by stress and trauma.
Some key influences include:
the ACE Study by Felitti and Anda, which demonstrates the link between childhood adversity and later addiction²
somatic approaches to trauma therapy, including Peter Levine’s Waking the Tiger³ and Bessel van der Kolk’s The Body Keeps the Score⁴
Stephen Porges’ Polyvagal Theory, which explains how the nervous system reacts to safety and danger⁵
the “Window of Tolerance,” introduced by Daniel Siegel, which helps clarify why overwhelm and shutdown happen when stress exceeds capacity⁶
Understanding Our Nervous System
The Vortex Model of Addiction is based on understanding how the nervous system reacts to stressful and traumatic experiences.
The nervous system is our primary operating system—our body’s command center. However, many of us know very little about how it functions, what it does, or what happens when it becomes overwhelmed.
Our nervous system influences:
thoughts
emotions
memory
sensations
behaviors
reactions
movement
bodily functions
instincts
It also shapes something many people don’t realize: how safe or unsafe we feel inside ourselves.
Much of what causes distress originates from internal signals—such as tightness, agitation, numbness, heaviness, or a sense of alarm—before we even put it into words. This is one reason why addiction can feel so confusing: the desire to use is often driven by internal experiences, not conscious choices.
The Autonomic Nervous System (ANS)
One of the most important divisions of the nervous system is the autonomic nervous system (ANS). The ANS manages involuntary body functions like digestion, temperature regulation, and heart rate. It also governs instinctive reactions when we sense danger.
Much of the ANS works outside of our conscious awareness. We don’t need to think about digesting lunch. Our body regulates temperature automatically. Similarly, the ANS responds automatically to threats without involving the thinking brain. For example, when we touch something hot, our hand quickly pulls away before we even realize what happened.
The ANS also plays a key role in how we respond to trauma and stressful events.
Why Biology Matters in Addiction
Understanding biology is essential for making sense of stress, trauma, and addiction. Adverse life events challenge our ability to maintain physical, emotional, mental, and relational health. When stress becomes chronic—or when trauma occurs—our nervous system can become dysregulated.
As a result, regulating emotions, behaviors, thoughts, and relationships becomes significantly more difficult. Trauma and chronic stress often create a foundation for turning to substances or certain behaviors as coping mechanisms. Mood-altering substances or actions become a way to regulate internal experiences when the nervous system has lost its ability to restore balance on its own.
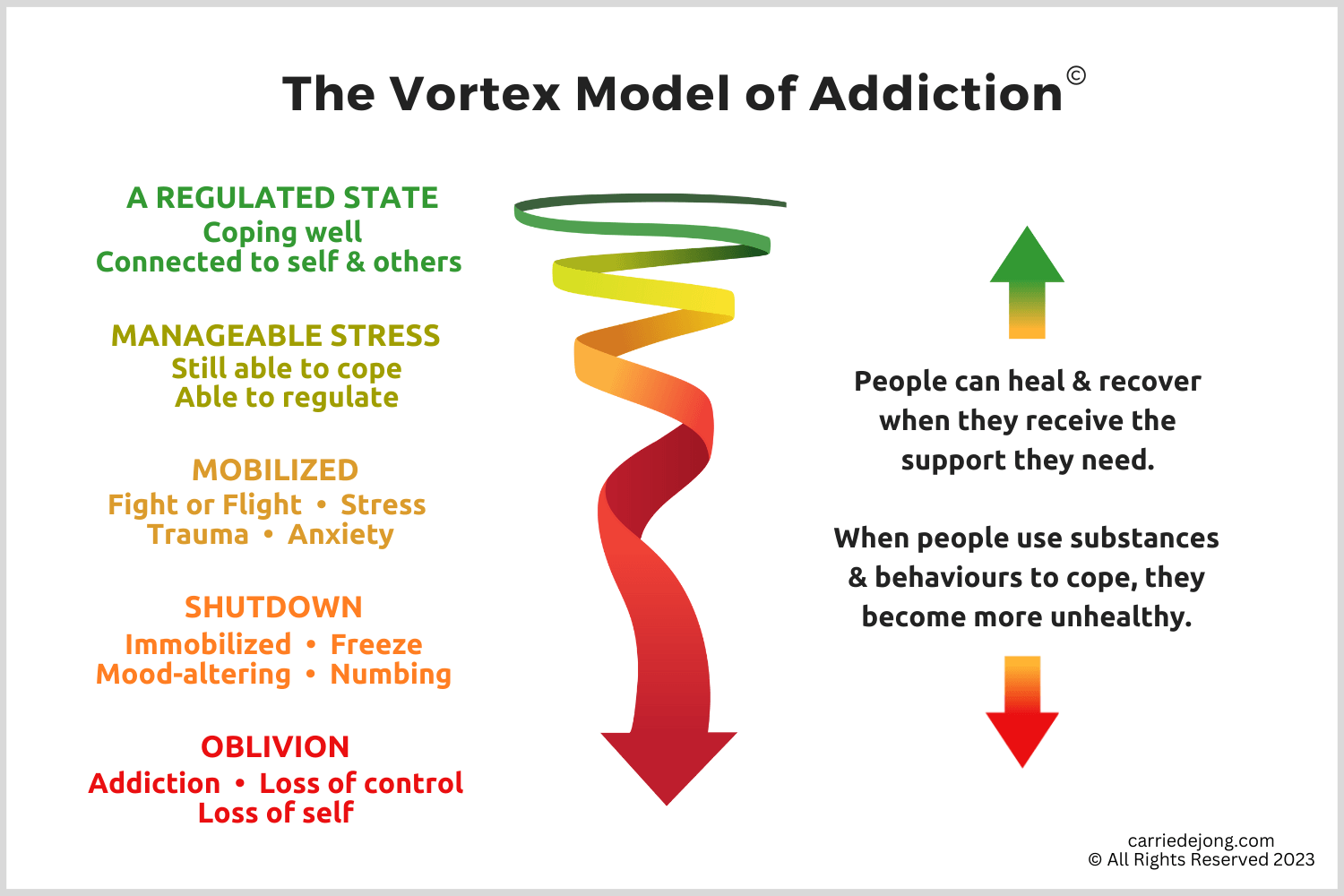
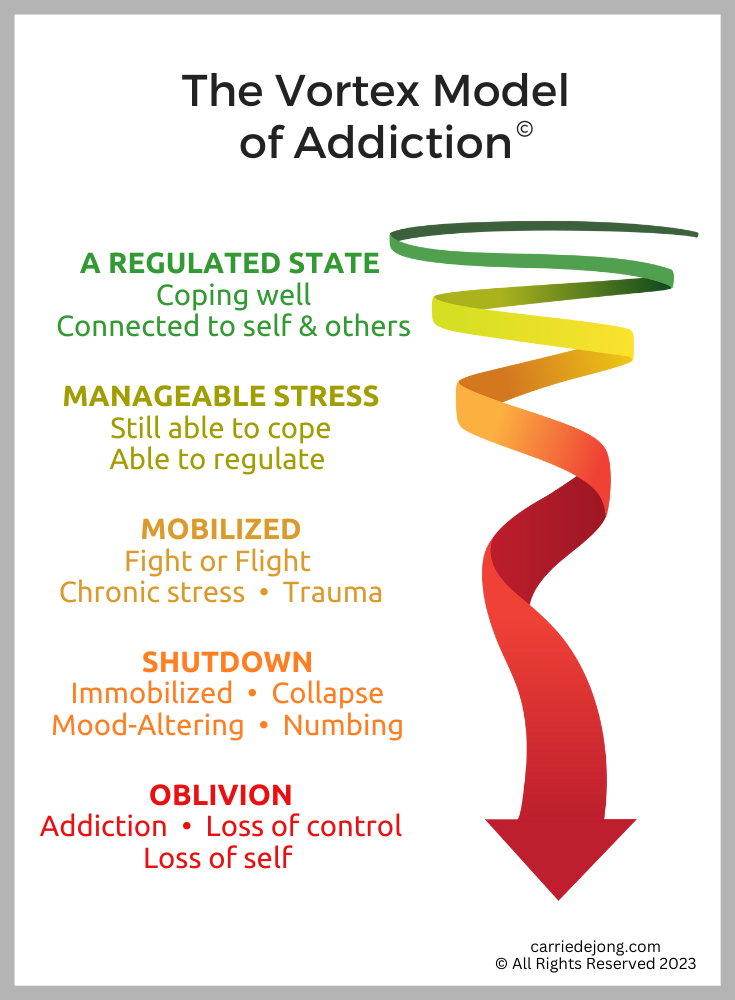
The Vortex Model of Addiction
So far, I’ve provided foundational information about the nervous system. This understanding is essential for the Vortex Model of Addiction.
Next, I outline five categories of nervous system functioning. These generally follow the states described in Polyvagal Theory.⁵
This model explains:
the progressive nature of addiction
the progressive nature of trauma symptoms
the process of recovery
1) A Regulated State
We function best when most aspects of life feel manageable. We are healthiest when the nervous system is regulated—when we can cope with stressors but still return to calm and restoration.
A regulated state includes the ability to:
care for our physical bodies
enjoy healthy relationships
regulate emotions and reactions
demonstrate clear thinking and judgment
make values-aligned choices
cope with everyday challenges
People who find regulation more accessible often:
address issues in their lives
participate in supportive relationships
engage in meaningful work or community
have a healthy repertoire of coping skills
reach out for support when needed
Many people who misuse substances or engage in mood-altering behaviors find it difficult to access this regulated state consistently. Those who experience addiction disorders rarely experience a true sense of calm.
2) Manageable Stress
Life doesn’t stay calm—and it isn’t meant to. Our modern lives bring countless sources of stress: deadlines, traffic jams, illness, conflicts, and pressure. Some stress can even be positive. Falling in love, learning new skills, or giving a speech increases demands on the nervous system.
When people are well-regulated, they can handle stressful situations and return to calm afterward. A good meal, connection with a loved one, exercise, or sleep helps “reset” the system. Their nervous system remains flexible enough to navigate in and out of challenges without getting stuck.
But life doesn’t always stay manageable. This is often where the journey into addiction begins.
3) Mobilized
If only life remained manageable — but it clearly doesn’t. We live in a world of constant busyness, nonstop stimulation, and ongoing pressure. Many people operate in a state of perpetual mobilization: stressed, exhausted, and always “on.’ This is reflected in the rising rates of anxiety, burnout, and stress-related illnesses.
A mobilized state occurs when the sympathetic nervous system (SNS) is activated. The SNS is the part of the autonomic nervous system responsible for the fight-or-flight response. When stress triggers this system, cortisol and adrenaline are released, heart rate increases, blood pressure rises, and the body prepares to respond.
This makes sense when a bear is chasing us. However, it becomes much more challenging when the threat is chronic—like ongoing anxiety, conflict, or unresolved trauma. In a mobilized state, the body often feels loud: racing heart, tight chest, restless energy, digestive issues, tension, and insomnia.
Many symptoms of chronic stress and anxiety fall into this category:
excessive worry
overthinking
rapid heartbeat
gastrointestinal issues
irritability
decreased social connection
busyness
insomnia
overwhelming emotional reactions
Trauma and Mobilization (Hyperarousal)
Trauma also produces a highly mobilized state.
Accidents, illness, violence, abuse, neglect, disasters, and other traumatic events are common among those struggling with addiction. These experiences activate fight-or-flight response during the event. However, for many, the nervous system does not return to baseline after the danger has passed. When trauma remains unresolved, mobilization can persist for years—or decades.
Trauma researchers often describe two broad categories of trauma response:
hyperarousal (too much activation)
hypoarousal (too little activation, shutdown)
Mobilization includes many common hyperarousal symptoms:
Ongoing high alert
startle response
hypervigilance
irritability
emotional reactivity
impulsivity
insomnia
Physical symptoms
tension
digestive problems
sweating
elevated heart rate
uncomfortable sensations that don’t easily settle
Mental symptoms
“busy brain”
difficulty concentrating
obsessive or intrusive thoughts
overthinking
reduced impulse control
Emotional reactivity
heightened anxiety, fear, shame
difficulty regulating anger
defensiveness
seeing threat where none was intended
Re-experiencing symptoms
flashbacks
nightmares
intrusive images
Mood-Altering in the Mobilized State
Living in fight-or-flight mode is exhausting. It is distressing, painful, and difficult to maintain.
So, what happens when people lack the tools or resources to return to regulation? They start to self-medicate. Many individuals struggling with addiction are trying to cope with trauma symptoms, anxiety, and chronic stress. One way people “take the edge off” is by using substances or behaviors that keep them activated—but alter the experience just enough to feel different, numb, or less emotionally painful.
Examples of mood-altering in mobilization:
excess caffeine
stimulant use (cocaine, methamphetamines)
compulsive exercise
gaming
gambling
compulsive spending
compulsive sexual behaviors
high-risk activities
Another way people take the edge off is by disconnecting more fully—moving from mobilization into shutdown. This brings us to the next stage of the vortex.
4) Shutdown
We name it in many ways: numb, checked out, disconnected, shut down.
Think of phrases like:
drowning our sorrows”
“taking the edge off”
“feeling no pain”
While the language varies, the goal is often the same: to disconnect from what feels unbearable.
Shutdown can feel like relief—especially after prolonged mobilization. Some people want to feel “nothing” rather than “everything.” This is especially true when dealing with unrelenting painful thoughts, feelings, memories, or sensations.
Hypoarousal and Dissociation
For many trauma survivors, shutdown is not a choice; it is a response of the nervous system.
When trauma and stress become overwhelming, the system can shift into dissociation and disconnection. In Polyvagal Theory, this state is often called immobilization.⁵ If hyperarousal involves fight-or-flight reactions, hypoarousal is the freeze response. Hypoarousal results in a sense of disconnection—you feel or experience “too little.”
This may include:
Emotional numbness
detachment
emptiness
difficulty identifying emotions
automatic shutting down
Painful emotions
overwhelm
helplessness
despair
chronic shame (which can become immobilizing)
Relational withdrawal
isolation
avoidance of intimacy
difficulty trusting others
Physical symptoms
fatigue
exhaustion
low energy
reduced ability to sense the body clearly
Cognitive symptoms
forgetfulness
“spaced out” feeling
memory problems
difficulty thinking clearly
Behavioral symptoms
inability to cope with daily responsibilities
feeling frozen or shut down
Peter Levine describes dissociation as something that “helps make unbearable bearable.”³ It is an automatic protective response. However, if healing does not happen, shutdown can become a long-term way of coping.
Mood-Altering in Shutdown
There are generally two goals when people mood-alter in shutdown:
1) To stay numb
Substances like alcohol, cannabis, and opiates can increase disconnection and help people avoid uncomfortable internal experiences.
2) To feel something
Those who live in persistent numbness might turn to high-risk activities or stimulating substances to feel alive, engaged, or activated. Behavioral addictions—such as gambling, compulsive sex, or risky acts—can also serve this purpose.
Regardless of the goal, the outcome is often the same: a destructive cycle that pulls someone deeper into the vortex.
Consequences of Shutdown
Although being shut down may feel “better” than mobilization, it is not healthier. Ongoing disconnection often means a person is no longer engaging in activities and relationships that support regulation, connection, and recovery.
Those who are consistently shut down often struggle with:
poorer physical and mental health
strained relationships
difficulty regulating emotions and actions
impaired judgment and thinking
reduced ability to cope with everyday life
When people attempt to disconnect from the painful impacts of unresolved trauma through substances or compulsive behaviors, it creates a fast transition into addiction—and its consequences. This brings us to the final stage of the vortex.
5) Oblivion
Out of control. Rock bottom. End-stage addiction. Oblivion.
“Oblivion” isn’t a clinical term, but it describes something real: the detachment that occurs when addiction has taken over.
Oblivion reflects the experience of being disconnected from:
self
others
the future
and sometimes even reality
Oblivion may include:
chronic addiction
severe negative consequences
significant health decline
homelessness
withdrawal seizures
substance-induced psychosis
suicidal thoughts or behaviors
profound loss of identity and self
When someone reaches this stage, they often require significant intervention and support to help them regain stability. Without assistance, the outcomes can be devastating.
Loss of a Sense of Self
One of the most painful consequences of addiction is the loss of identity. Addiction causes a profound loss of control. People often keep using despite their intentions, values, and repeated promises to themselves and others. In active addiction, the ability to choose is greatly diminished.
For certain substances—especially alcohol, opiates, and benzodiazepines—physical dependence can also develop. Withdrawal symptoms may be severe and, in some cases, life-threatening.
Addiction can cause individuals to engage in behaviors they never thought possible. Important aspects of life are often neglected. Values and morals may be compromised. High-risk sexual activities might occur. Laws can be broken. Children could be neglected. Families suffer damage. People seldom set out to do these things. This is part of the heartbreak of addiction.
Over time, essential parts of self—confidence, self-esteem, motivation, hopes, and dreams can become more elusive. Substances and addictive behaviors also impair brain functioning. Concentration declines, cognition is affected, and personality changes can occur.
Emotional Costs
Mood-altering substances and behaviors reduce the ability to feel—this is one of the “benefits” people experience in the short term. But here’s the cost: while substances lessen painful emotions, they also decrease the ability to feel good in the long run.
Long-term substance use often increases anxiety. Irritability and resentment can build. Relationships become strained, especially when loved ones attempt to confront the addiction. Many people continue to use not to feel “good,” but to avoid feeling bad.
Shame is a common emotion in addiction. It’s that burning feeling of failure that makes someone want to withdraw and hide. As consequences build up, shame intensifies—and it can become a trigger for further mood-altering.
This creates a vicious cycle: shame → using → consequences → more shame.
Physical Health Is Compromised
Long-term substance use can severely compromise physical health, increasing risk of:
malnutrition
infections
liver disease
cardiovascular disease
substance-related brain damage
Alcohol addiction also involves serious withdrawal risks. Delirium tremens (DTs) is a dangerous form of alcohol withdrawal that can cause tremors, agitation, rapid heartbeat, and hallucinations. Quitting alcohol suddenly can lead to withdrawal seizures and other life-threatening issues.
Mental Illness Is Common
Chronic substance use and behavioral addictions have profound impacts on mental health. Some individuals start using substances to cope with anxiety or depression. However, addiction often worsens mental health symptoms over time, including panic, hopelessness, depression, and suicidal thoughts or behaviors.
Substance-induced psychosis can occur with cannabis, cocaine, or methamphetamines.
Although suicide is usually seen mainly as a mental health issue, its risk is closely linked to addiction disorders. Trauma and PTSD also elevate suicide risk. Addiction to drugs and alcohol increases the likelihood of suicide tenfold. Suicide rates among polydrug users (those using more than one substance) are up to 17 times higher than in the general population.
Increased Risk of Additional Trauma
There are many sources of trauma within addiction itself. Even if someone views these consequences as “choices,” they are no less traumatic because they happen in the context of addiction.
Additional trauma may include:
falls, injuries, accidents
serious health issues caused by substance use
significant losses
violence or sexual trauma
overdoses
psychosis
seizures
We are also currently facing a crisis of opioid overdoses in North America. Accidental overdoses have surged significantly, especially with fentanyl. The use of multiple substances has also increased, leading to more unintentional overdoses and more serious physical and mental health issues.
Traumatic experiences experienced during active addiction increase the trauma load, which in turn heightens the need to use mood-altering substances to manage trauma symptoms.
Summing It Up
When someone reaches Oblivion, they often cannot break free from the addictive cycle on their own. Most people need intervention and support, such as:
medical care
addiction treatment
a recovery program
trauma-informed therapy
community and relational support
The possibility of hope and recovery does exist. Vortex of Addiction shows how trauma and stress can overwhelm the nervous system. When we don’t have adequate support or resources to recover, mood-altering often becomes a way of coping—but it disconnects us from the very things that help us heal.
One of my beliefs as an addiction therapist is that “the problem is the problem.” Addictive patterns are often a symptom of unresolved trauma or chronic stress—not simply the “problem” itself.
For anyone struggling with addiction, it is essential to find qualified support that addresses both:
the addiction
and the overwhelming life experiences that created the desire to numb, disconnect, or escape
Trauma-informed care understands that safety and compassion are fundamental to healing and recovery—especially when trauma is involved.
Thank you for your interest in the Vortex Model of Addiction. This model not only explains the journey into addiction but also describes the path back: the gradual process of returning to regulation, connection, and self-awareness.
Continue Exploring
An overview of the Vortex of Addiction and the patterns that sustain addiction and recovery.
How addictive patterns can shift between behaviors.
Why cravings feel so powerful and persistent.
References
1. U.S. Surgeon General. Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health.
2. Felitti, V. J., Anda, R. F., et al. “Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults.” American Journal of Preventive Medicine, 1998.
3. Levine, P. A. Waking the Tiger: Healing Trauma. 1997.
4. van der Kolk, B. The Body Keeps the Score. 2014.
5. Porges, S. W. Clinical Applications of the Polyvagal Theory. 2018.
6. Siegel, D. J. The Developing Mind. 1999.
7. Langeland, W., Draijer, N., & van den Brink, W. “Trauma and Dissociation in Treatment-seeking Alcoholics.” Comprehensive Psychiatry, 2002.