
Treating Trauma and Addiction Together: What Clinicians Need to Know
When trauma and substance use co-occur, the most effective treatment supports both—without overwhelming the client.
When a client is struggling with both trauma symptoms and substance use, the question isn’t “Which one matters more?” The question is: What will help them stabilize enough to stay alive, stay engaged, and begin healing?
Many clinicians have heard the phrase: “Always deal with the alligator closest to the boat.” In addiction treatment, that “alligator” often refers to the substance being used. And sometimes, that’s completely accurate—especially when withdrawal risk, overdose risk, or immediate safety concerns are involved.
However, relying too much on that idea can be problematic: if trauma is fueling the addiction, treating substance use without addressing trauma usually leaves clients with the same problem but fewer coping tools.
The Reality: Trauma and Addiction Overlap More Than We Like to Admit
Research consistently shows high rates of trauma symptoms among individuals seeking treatment for substance use disorders.
• In the general population, lifetime PTSD rates are often estimated at about 7%.
• In addiction treatment settings, PTSD rates are much higher, often ranging from 36% to 50%.
• People with PTSD also face a significantly increased risk of developing substance use problems.
Even when someone doesn’t meet full the PTSD criteria, trauma-related symptoms—hypervigilance, emotional flooding, dissociation, shame, and chronic anxiety—can still influence the addiction cycle.
In other words, many clients aren’t just “using.” They’re coping.
Why This Question Matters So Much
When trauma and addiction coexist, treatment can easily become disjointed:
Trauma programs often struggle to work with clients who are actively using substances.
Addiction programs often emphasize abstinence but may not sufficiently address trauma.
Mental health clinicians may feel unprepared for relapse, withdrawal, or high-risk substance use.
Addiction clinicians might not feel equipped to safely assess trauma symptoms.
Clients often bounce between systems that each address only part of their story. And the client bears the burden of integrating these parts on their own.
The Core Problem With “Pick One First”
Historically, many treatment systems have addressed trauma and addiction as separate tracks. However, for most clients, these aren’t separate issues; they are mutually reinforcing.
Trauma symptoms increase the urge to numb.
Substance use increases dysregulation, shame, and emotional instability.
Both reduce self-regulation capacity.
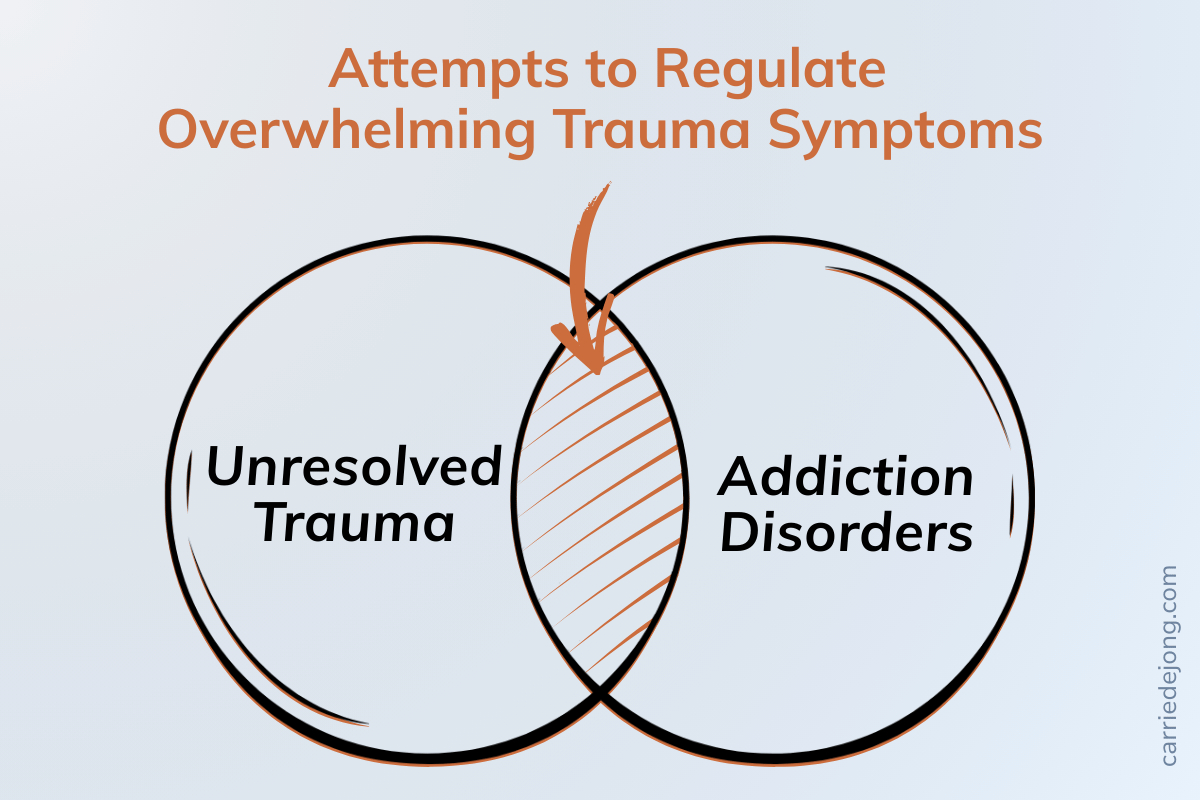
Both increase the risk of relapse. This is often described as mutual maintenance—each condition sustains the other.
A More Helpful Clinical Question
Instead of asking: “Should we treat trauma or addiction first?” a better question is: “What does this client need to become more stable and less overwhelmed?”
Because for many clients, substance use is not the original problem. It’s the attempt to manage:
intrusive memories
emotional flooding
panic and hyperarousal
numbness and shutdown
chronic shame
insomnia
loneliness and disconnection
unbearable body-based distress
What “Stabilization” Actually Means (In Plain Language)
Stabilization is not avoidance. And it is not “ignoring trauma.” Stabilization means helping a client build enough safety and internal regulation that they can:
tolerate distress without spiraling
stay present in sessions
remain engaged in treatment
reduce self-destructive behaviors
begin building healthier coping tools
reduce relapse risk
For many clients, stabilization is trauma treatment. It just isn’t trauma processing yet.
Why Trauma-Informed Addiction Treatment Is Not Optional
Many addiction programs say they are trauma-informed. But often, that means only:
softer language
less confrontation
a general awareness that trauma exists
That’s a start—but it’s not enough. Trauma-informed addiction treatment needs to include practical clinical shifts, such as:
understanding dissociation and shutdown
recognizing trauma triggers that drive cravings
working with shame as a central mechanism (not a side effect)
teaching nervous-system-based regulation skills
avoiding interventions that increase fear, humiliation, or powerlessness
supporting emotional safety in group settings
Without this, clients are often treated as if their symptoms reflect “resistance” rather than dysregulation.
Why Some Clients Don’t “Seem Ready” (But Actually Are)
One of the most damaging clinical misinterpretations happens when trauma symptoms are mistaken for:
unwillingness
denial
lack of motivation
“not hitting bottom”
manipulation
resistance
For example:
A client who becomes defensive may be experiencing threat activation.
A client who shuts down may be dissociating.
A client who relapses after treatment may be overwhelmed by trauma symptoms once substances are removed.
When we interpret trauma-based survival responses as moral or motivational failures, we create shame. And shame is one of the most powerful relapse triggers there is.
The Myth That Trauma Can’t Be Addressed Until Abstinence
A common belief in both addiction and trauma treatment is: “You can’t do trauma work until the client has a stable period of sobriety.” Sometimes, this is clinically true—especially when a client is highly intoxicated, medically unstable, or unable to remain present.
But for some, that can become a setup for failure. Because what we’re often asking is: “Give up the one thing that reliably reduces your distress… before we teach you anything else that works.”
Many clients simply cannot do that. Not because they don’t want recovery badly enough. But because their nervous system doesn’t yet have other ways to cope.
So What Should Clinicians Focus on First?
Here’s the most accurate answer: Focus on stabilization and integration.
Not trauma vs. addiction.
Not abstinence vs. processing.
Not “alligator first” as a one-size-fits-all rule.
Instead:
Address immediate safety.
Build regulation skills.
Reduce shame.
Support connection.
Treat both conditions as part of the same system.
What Integrated Treatment Actually Looks Like
Integrated treatment doesn’t mean you dive into detailed trauma processing on day one.
It means you begin addressing trauma safely by:
naming the trauma–addiction link
teaching clients how dysregulation works
helping them identify triggers and body cues
building coping tools for distress tolerance
supporting emotional regulation and relational safety
creating a plan for trauma therapy when readiness increases
This approach reduces dropout risk and increases long-term recovery outcomes.
In Summary
If you’re a clinician working with trauma and addiction, the most helpful stance is not: “Which should I treat first?” Instead, ask: “How do I help this person become safer, steadier, and more supported—so they can heal both?”
Because the truth is simple: Trauma and addiction are often part of the same survival story. And healing works best when we treat them that way.
Continue Exploring
How trauma responses can influence addiction and relapse patterns.
The ACE Study: How early trauma shapes coping and addiction.
Understanding interoception and how internal awareness and support regulation and healing.